The term “golden hour” is borrowed from emergency medicine, where it describes the critical window immediately following trauma when rapid, correct intervention most dramatically affects the probability of survival. In commercial pig production, the concept applies with equal precision to the first 60 minutes of a newborn piglet’s life — a window during which the physiological vulnerabilities that kill more piglets than any other cause are simultaneously present, simultaneously addressable, and simultaneously time-sensitive in a way that makes this single hour the most consequential management window in the entire production cycle.
A piglet arrives in the world with four simultaneous challenges: it must transition from fetal physiology (oxygen delivered via placenta, temperature maintained by the uterine environment, nutrition delivered through the umbilical cord) to independent physiology (breathing air, thermoregulating independently, sourcing nutrition from milk). Each of these transitions has a specific failure mode — birth asphyxia, hypothermia, colostrum deprivation, and crushing — and each failure mode has a specific, rapid-response intervention that addresses it within the golden hour before it becomes irreversible.
What makes the golden hour distinct from other critical management windows is the brevity of the intervention window combined with the irreversibility of missed interventions. A piglet with body temperature below 35°C within the first hour of life is entering a hypothermic spiral that suppresses the suckling reflex, preventing the colostrum intake that would provide both energy and antibody protection — creating a cascading physiological failure that is increasingly difficult to reverse the longer it is allowed to develop. A piglet born with fluid partially obstructing its airways that does not receive the 30-second intervention to clear them may never establish adequate ventilation and will die in the first hour regardless of every subsequent intervention.
This guide provides the complete golden hour protocol — the specific interventions, their correct technique, their precise timing within the hour, and the prioritization logic that determines which intervention takes precedence when multiple piglets require simultaneous attention.
The Physiology of the First Hour — Understanding What the Newborn Piglet Faces
The Respiratory Transition
During fetal life, the piglet’s lungs are fluid-filled — the respiratory system is physically developed but functionally dormant. Gas exchange occurs entirely through the placenta, with the umbilical circulation carrying oxygenated blood from the dam to the fetus and returning deoxygenated blood for placental gas exchange.
At birth, three things must happen within the first few minutes for the piglet to establish successful independent respiration:
- Lung fluid must be expelled or absorbed: The mechanical compression of the thorax during passage through the birth canal expels a significant portion of lung fluid — this is why the sudden passage through the birth canal, and the brief compression it creates, is actually beneficial for respiratory establishment. Piglets delivered by caesarean section, bypassing this compression, are at higher risk of initial respiratory difficulty for exactly this reason.
- The first breath must be taken: The drop in oxygen and rise in carbon dioxide that occurs as umbilical circulation is interrupted (as the umbilical cord stretches and eventually separates) triggers the respiratory center in the brainstem to initiate the first independent breath. This happens within seconds to 1–2 minutes of birth in healthy piglets — delayed beyond this window indicates birth asphyxia requiring intervention.
- Pulmonary circulation must shift from fetal to neonatal pattern: In fetal life, most blood bypasses the non-functional lungs through the foramen ovale and ductus arteriosus — these shunts close in response to the rise in arterial oxygen that accompanies successful first breaths. A piglet that does not establish adequate ventilation cannot trigger this circulatory shift — creating a cycle where inadequate oxygenation perpetuates inadequate circulation and vice versa.
The Thermal Challenge
The newborn piglet’s thermal situation is acutely precarious for three simultaneous reasons:
High surface-area-to-body-mass ratio: At 1.2–1.5 kg average birth weight, the pig is small relative to most other domestic livestock species at birth, and small body size means proportionally more heat-dissipating surface relative to heat-generating body mass.
Minimal insulating subcutaneous fat: Unlike older pigs (and unlike some other neonatal species), the newborn piglet has minimal subcutaneous fat to insulate against heat loss — the fat deposition that creates meaningful thermal insulation develops over the first weeks of life, not before birth.
Wet at birth: A newborn piglet emerging through the fluid-filled birth canal is wet — and wet skin loses heat through evaporation at a rate many times greater than dry skin. The body temperature of a newborn piglet in a 20°C environment can drop 3–4°C within the first 10 minutes of birth if not dried promptly.
The consequence: At ambient temperatures below the piglet’s thermoneutral zone (32–34°C in the first days of life), every minute without adequate thermal support represents measurable body temperature decline. A piglet with core body temperature below 35°C shows suppressed suckling reflex — it cannot nurse effectively even if physically capable of reaching a teat. Below 34°C, physiological compromise becomes more severe. Below 32°C, the prognosis without active rewarming intervention becomes poor.
The Colostrum Dependency
The newborn piglet has essentially no immunological protection from birth — it arrives immunologically naive, without the transplacental antibody transfer that some other mammalian species receive, because the pig’s epitheliochorial placenta does not allow antibody passage. Its entire early-life antibody supply comes from one source: colostrum, the antibody-rich secretion from the sow’s mammary glands in the hours immediately following farrowing.
Two critical time factors compound the urgency of colostrum intake:
Colostral antibody concentration declines rapidly: The immunoglobulin concentration in colostrum is highest in the first 6–12 hours after farrowing and declines substantially thereafter as normal milk progressively replaces colostrum. A piglet that nurses at 8 hours of age receives substantially less antibody protection than one that nursed at 1 hour of age.
Intestinal absorption capacity closes rapidly: The piglet’s small intestine is capable of absorbing intact immunoglobulin molecules (large proteins that would normally be digested) directly into the bloodstream only for the first 24–36 hours of life — this window of “gut closure” narrows rapidly, and immunoglobulins consumed after gut closure are digested rather than absorbed, providing nutritional but not immunological benefit.
The minimum adequate colostrum dose: Research indicates that a piglet requires approximately 250–300 mL of colostrum in the first 24 hours of life for adequate passive immunity transfer — equivalent to approximately 4–6 nursing bouts of adequate duration and intake during this period.

Intervention 1 — Airway Clearance and Respiratory Stimulation
The Assessment: Is the Piglet Breathing?
The first assessment for every piglet immediately upon birth: is it breathing? This determination should take no more than 3–5 seconds:
- Breathing adequately: Chest movement visible, regular rhythm, piglet showing initial orientation and movement responses. Move directly to drying and thermal management.
- Breathing weakly or irregularly: Shallow, infrequent chest movement, limited movement responses, pale or mottled coloring. Proceed to airway clearance and stimulation immediately.
- Not breathing: No visible chest movement, limp, possibly pale-to-blue coloring. This is a respiratory emergency requiring immediate intervention.
Airway Clearance
For any piglet showing inadequate respiration, the first intervention is clearing the airways:
Step 1 — Remove membranes: Clear any birth membranes (fetal membrane remnants) from the face and nostrils — occasionally a piglet emerges still partially enclosed in the amniotic sac, which must be immediately broken and removed from around the face and nostrils.
Step 2 — Wipe the nose and mouth: Using a clean dry cloth, wipe the nostrils and oral cavity to remove fluid and mucus — the mechanical action of wiping also provides facial stimulation that helps trigger the respiratory reflex.
Step 3 — Bulb syringe (where available): A small bulb syringe inserted gently into each nostril and squeezed to create suction, then released, draws fluid from the upper respiratory tract more effectively than wiping alone. For farms where farrowing attendance is standard, keeping a small bulb syringe in the farrowing kit (as detailed in the first-aid kit guidance in this series) is a worthwhile low-cost addition specifically for this purpose.
Respiratory Stimulation Techniques
Vigorous towel rubbing: The most accessible and generally most effective first stimulation — firm, rapid rubbing of the piglet’s entire body with a clean dry towel, with particular attention to the chest and ribcage area. The mechanical stimulation of rubbing stimulates both the respiratory center (through sensory input from skin mechanoreceptors) and circulation (through the friction-induced warmth and circulatory stimulation). This technique is effective, safe, and requires no specialized equipment.
The head-down position: Hold the piglet with its head lower than its body, supporting it firmly by the hindquarters — gravity assists in draining fluid from the upper airways while the chest-down orientation facilitates drainage from the lungs themselves. Combine with brisk rubbing of the back and sides in this position for 15–20 seconds before assessing breathing response.
The swinging technique (for experienced handlers only): A controlled swinging motion — holding the piglet securely with one hand cupping the head/neck and the other supporting the hindquarters, and performing a brief arc swing from above the handler’s head to below waist level (2–3 repetitions) — uses centrifugal force to help expel airway fluid that is obstructing ventilation. This technique is effective but requires appropriate technique to avoid injury — the piglet’s head and neck must be firmly supported throughout, and the swing must be controlled and deliberate rather than vigorous or jerky. It is best learned through direct demonstration from an experienced farrowing attendant rather than from written description alone.
Sternum rubbing: Firm pressure applied with the thumb or two fingers to the sternum (breastbone) in a rubbing motion stimulates the chest wall mechanoreceptors adjacent to the heart and large vessels — a targeted version of the general rubbing stimulation that may be more effective for piglets that have not responded adequately to general body rubbing.
The Assessment After Stimulation
After 30–60 seconds of stimulation, reassess:
- Is chest movement now present and regular?
- Is the piglet showing limb movement and orientation responses?
- Is skin color improving from pale or blue toward pink?
A piglet that has responded well should be proceeding toward drying and thermal management. A piglet that has not responded to 60 seconds of stimulation warrants continuing efforts while managing the logistical reality that other piglets in the same litter are being born and also require attention — in practice, an assistant or the ability to briefly set a non-responsive piglet in a warming area while attending to other births and returning to it is the field management reality.
Intervention 2 — Drying and Thermal Management
Why Drying Is Both a Thermal and a Stimulatory Intervention
Towel drying of the newborn piglet serves two simultaneous functions: it removes the moisture from the birth fluids that is causing rapid evaporative heat loss, and the mechanical rubbing action of thorough drying provides the sensory stimulation that promotes respiratory function and circulatory activity — making it one of the most physiologically efficient interventions available, addressing two of the four major neonatal vulnerabilities simultaneously.
Drying technique:
- Use a clean, dry cloth or paper towel — pre-warmed if possible (keeping drying cloths in the creep area where they absorb warmth from the heat lamp makes each drying action itself thermally beneficial rather than thermally neutral)
- Dry the entire body surface, with particular attention to the head (including inside the ears, where moisture retention contributes to heat loss and provides an entry point for environmental bacteria) and the feet (where the large surface area relative to tissue mass creates disproportionate heat loss)
- Dry vigorously — this is not a gentle procedure; the stimulatory value comes from the mechanical friction, not from careful handling
Moving to the Heat Source
Immediately after initial drying, move the piglet to the warmed creep area — the zone of the farrowing crate maintained at 32–34°C by the heat lamp or heating pad.
Why speed matters: A piglet that has been partially dried but remains on the farrowing crate floor (typically at ambient temperature, 22–26°C in a well-managed farrowing house) is still losing body heat, just more slowly than when wet. Every minute between birth and reaching the heat source represents continued body temperature decline from an already-compromised baseline.
The heat source verification: The importance of verifying that the heat source is functioning and at the correct temperature before farrowing begins — not reactively checked when the first piglet arrives — cannot be overstated. A heat lamp that burned out during the previous night, or a heating pad connection that came loose, creates a situation where piglets are being placed on a floor at ambient temperature that they cannot distinguish from a functional heat source until their body temperature has already declined significantly.
Thermal Assessment
A piglet placed in a correctly functioning warm creep area (32–34°C) should show progressively increasing activity over the first 15–20 minutes — initially lying still or showing limited movement, then becoming more active, making standing attempts, vocalizing (the characteristic short grunting call that indicates the piglet is actively seeking the udder), and orienting toward the udder side of the crate.
Signs of inadequate thermal management (hypothermia developing):
- Persistent limpness and inactivity beyond 15–20 minutes in the warm creep
- Failure to respond to being placed against the udder — no suckling attempts or weak, ineffective attempts
- Pale to bluish skin color (cyanosis from peripheral vasoconstriction as the body prioritizes core temperature at the cost of peripheral circulation)
- Cold feel to the ears and extremities
Response to developing hypothermia:
A piglet showing signs of hypothermia within the first hour requires active rewarming rather than passive placement in a warm area:
- Direct body contact with a warm heat pad at approximately 38–40°C (wrapping the piglet in a warm towel warmed on the heat lamp, or placing it directly on the warming pad surface)
- In severe cases where rapid rewarming is needed: immersion of the body (keeping the head above water) in warm water at 38–40°C for 3–5 minutes — this is the most efficient rapid rewarming method available without specialized equipment, transferring heat to the piglet’s core far faster than air warming alone
After rewarming: Thoroughly dry the piglet again (particularly important after water immersion), then place it against the udder for assisted nursing — a successfully rewarmed piglet that still cannot nurse because it lacks energy for active suckling may benefit from a small amount of manually expressed colostrum dripped onto its lips to provide both the sucrose stimulus and immediate energy support.
Intervention 3 — Navel Care
The Umbilical Cord as an Infection Pathway
The umbilical cord stump represents an open pathway from the external environment to the piglet’s systemic circulation — a direct route for environmental bacteria to enter the bloodstream before the immune system (still dependent entirely on colostral antibody for protection) is equipped to respond.
The most common consequence of inadequate navel care: Navel ill (omphalitis) — infection of the umbilical stump that can progress to systemic septicemia, joint infections (neonatal arthritis — “joint ill”), and meningitis in severe cases. Beyond the direct clinical consequences, subclinical navel infection diverts the piglet’s early immune resources toward managing an avoidable bacterial challenge at the moment those resources are most limited and most needed for protection against other environmental challenges.
Navel Care Protocol
Timing: Within the first 30 minutes of birth, after initial drying and respiratory assessment.
Materials: Iodine solution (povidone-iodine, 10% concentrated, diluted to 0.5–1% working solution is more appropriate for navel dipping than full-strength solution) in a small navel dipping cup — a container small enough to fully submerge the navel stump in a single dipping action.
Technique:
- Allow the umbilical cord to naturally separate if it has not already — most cords separate naturally during or shortly after birth; do not prematurely cut the cord unnecessarily, as the natural separation point is further from the body wall than a cut cord, leaving a longer stump that is less likely to cause navel infection from proximity to the body wall
- If the cord is excessively long (more than 5–6 cm) or still intact with the placenta, cut with clean scissors or a cord clamp at approximately 3–5 cm from the body wall
- Dip the entire navel stump in the iodine solution — completely submerging it in the cup, holding for 5–10 seconds to allow contact between the disinfectant and the entire stump surface and the skin junction where it meets the body wall
- Allow to air dry — do not wipe or rinse
Repeat dipping: A second navel dip at 12–24 hours of age provides additional protection during the period when the stump is drying and constricting but before it has fully desiccated into a dry, less permeable state.
Intervention 4 — Ensuring First Colostrum Intake
The Priority Hierarchy Within the Golden Hour
Of all the golden hour interventions, ensuring that every piglet receives adequate colostrum in the first 1–2 hours of life is simultaneously the most important (in terms of long-term production consequences) and the most frequently inadequately managed (in terms of the systematic attention required to verify it has occurred for every piglet in a large litter).
The priority hierarchy within the golden hour, when multiple piglets need attention simultaneously:
- Respiratory support for any piglet not breathing — 60 seconds without adequate intervention may be fatal; this takes absolute priority
- Thermal protection — body temperature decline is rapid but a few minutes of prioritizing respiratory intervention first is acceptable
- Colostrum access — absolutely critical, but the window (first 1–2 hours) is long enough that the 5–10 minutes spent on respiratory and thermal interventions for one piglet will not typically compromise colostrum access if that piglet is placed promptly against the udder afterward
Assisting Colostrum Intake
For vigorous, normally-developing piglets: Once dried and warmed, most healthy piglets will find and latch onto a teat independently within 15–30 minutes. The role of the attendant for these piglets is primarily to confirm success — observing that the piglet has latched, is making active suckling movements, and appears to be swallowing.
For smaller or weaker piglets: Direct assistance is required — physically guiding the piglet to a teat (preferably one of the well-developed glands producing freely expressible colostrum) and supporting it in position until it latches and establishes suckling. For piglets too weak to maintain the suckling posture independently, cupping the hand beneath the piglet to support its body while it nurses allows suckling without the piglet spending energy it cannot spare on maintaining its own position.
For piglets failing to nurse despite position assistance: Where a piglet cannot achieve adequate suckling despite assistance, manual colostrum administration via syringe — drawing colostrum expressed from the sow (or from a frozen colostrum reserve, if the farm maintains one) and carefully dripping it into the piglet’s mouth at a rate the piglet can swallow without aspiration — provides a bypass for the first critical colostrum dose. Tube feeding (passing a small feeding tube through the mouth and into the stomach) is the most reliable method for delivering a known colostrum volume to a piglet that cannot nurse independently, though it requires training to perform safely and is most appropriate for stockpersons who have had this technique specifically demonstrated.
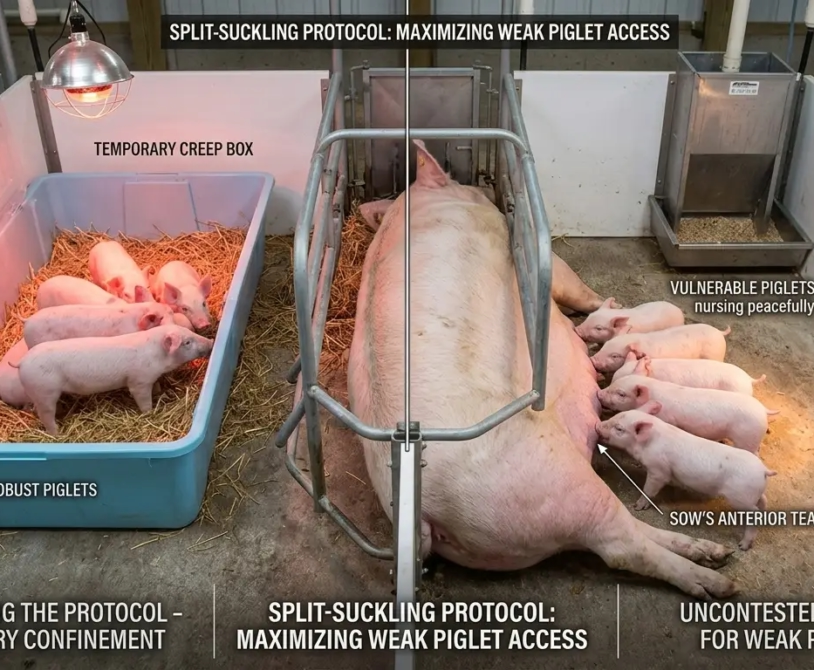
The Split-Suckling Technique for Large Litters
As introduced in the farrowing management handbook, split-suckling — temporarily confining larger, more vigorous piglets in the warm creep area while smaller, weaker litter members have uncontested access to the sow’s teats — ensures that the most vulnerable piglets in large litters receive adequate first colostrum intake without being displaced by their stronger siblings.
Practical split-suckling within the golden hour:
- After the entire litter has been born, dried, and placed in the creep area, identify the largest 30–40% of piglets by visual size estimation
- Return only the smaller piglets to the udder for a period of 30–45 minutes — giving them uncontested access to the highest-producing teats (typically the anterior glands closest to the forelegs) without competition from larger littermates
- After this period, allow the full litter free access to the udder
- Monitor to ensure smaller piglets have genuinely nursed during their uncontested access period — a small piglet placed at the udder that does not successfully latch and nurse during this window requires additional individual intervention
Intervention 5 — The 8-Hour Assessment
Why 8 Hours Is the Critical Checkpoint
While the most acute golden hour interventions occur in the first 60 minutes, the 8-hour assessment is the checkpoint that confirms the golden hour’s interventions have resulted in sustainable outcomes — that each piglet has successfully transitioned to independent thermal management and established the regular nursing pattern necessary for ongoing energy and antibody intake.
The 8-hour crop fill equivalent: As referenced in brooding management guidance for poultry (and applicable by analogy to the pig nursling), the 8-hour assessment in the farrowing house is the checkpoint that provides the most reliable early indicator of successful transition:
For each piglet, assess:
- Body condition: A well-fed piglet at 8 hours of age has a visibly rounded, full abdomen — milk in the stomach produces a characteristic plumpness visible particularly in the dorsal-to-ventral profile. A thin, sunken abdominal profile at 8 hours indicates inadequate milk intake and requires investigation and intervention.
- Activity level: Alert piglets that have nursed adequately will be active when disturbed, responsive to handling, and will actively seek the udder when placed against the sow’s flank. Persistently lethargic or weak piglets at 8 hours require individual assessment.
- Body temperature: A piglet that has successfully established thermal homeostasis will feel warm to the touch across its back and flanks. A persistently cool or cold piglet at 8 hours indicates continued thermal support failure.
- Skin color: Pink skin coloring across the body surface indicates adequate oxygenation and peripheral circulation. Pale or mottled skin indicates circulatory compromise.
What to do when the 8-hour assessment identifies a problem:
A piglet identified as thin, lethargic, cool, or pale at 8 hours is in a precarious state — inadequate colostrum intake has compromised both energy reserves and immune protection simultaneously, and the window for effective intervention is not unlimited:
- Warm the piglet if necessary (hypothermia underlies many cases of inadequate 8-hour development)
- Administer colostrum directly — manually expressed from the sow or from frozen colostrum reserve — via syringe or feeding tube, targeting a minimum 25–30 mL dose
- Place the warmed, colostrum-dosed piglet against the sow’s udder in a supported position and observe for successful latching
- Reassess at 2-hour intervals until the piglet shows sustained improvement

The Colostrum Reserve — Building Farm-Level Insurance
Why Frozen Colostrum Has a Place in Every Farrowing Operation
The scenarios where frozen colostrum reserves provide direct life-saving value occur in every farrowing house eventually:
- A sow dies during or immediately after farrowing, before her litter has received adequate colostrum
- A sow’s colostrum production is compromised by MMA complex within the first hours after farrowing
- An orphaned or excessively large litter exhausts available nursing capacity before every piglet has nursed adequately
- A weak piglet that cannot nurse independently requires direct colostrum administration to survive the first critical hours
Building a colostrum reserve:
Colostrum can be collected from high-milk-producing sows with litter sizes smaller than their teat count allows — the “excess” teats that would otherwise not be suckled can be gently hand-milked during the farrowing and early lactation period, with the collected colostrum stored in small labeled containers (10–15 mL per container is a practical individual dose unit) in the farm freezer.
Frozen colostrum management:
- Freeze within 1 hour of collection to preserve immunoglobulin concentration
- Label with collection date and, where possible, the collecting sow’s vaccination status (higher-value colostrum from sows with recent vaccination against specific pathogens)
- Thaw at 40°C maximum (body temperature) — not in boiling water or microwave, which denatures the antibody proteins and eliminates the immunological value while preserving only the nutritional content
- Use within 24 hours of thawing
- Maintain a rotating stock with a maximum 6-month storage period — immunoglobulin potency declines with extended frozen storage
Managing Multiple Births Simultaneously — The Real-World Challenge
The Problem of Parallel Demands
The ideal golden hour protocol assumes the capacity to give each piglet immediate, sustained individual attention. In practice, a sow may deliver her next piglet every 15–20 minutes, creating 3–4 births in the first hour, each of which simultaneously needs drying, respiratory assessment, navel care, and placement at the udder — while the previous birth’s piglet may not yet have successfully nursed.
The triage framework for multiple simultaneous demands:
Immediate action (any piglet): Breathing status and airway clearance — 30 seconds maximum; no other demand takes priority
High priority (within first 5 minutes): Drying and thermal placement — delayed drying of even 2–3 minutes while attending to another piglet is significant but recoverable; delayed drying beyond 10 minutes in typical farrowing house ambient temperatures creates meaningful hypothermia risk
Medium priority (within first 20 minutes): Navel care — important but not time-critical at the same scale as breathing and thermal management
Schedule-able (within first 60–90 minutes): Colostrum access verification and assisted nursing — the window is long enough to be managed after the acute interventions for all born piglets have been addressed
The two-person farrowing advantage: Where staffing allows, having two people present for a farrowing — one focused on attending to the sow (monitoring progression, assisting with dystocia if needed, recording birth time and order) and one focused on neonatal piglet processing (drying, respiratory stimulation, navel care, placement) — eliminates the parallel-demand management challenge entirely and represents the highest standard of golden hour care. For farms where two-person attendance is not consistently achievable, identifying the highest-value litters for that resource allocation (gilts farrowing their first litters, sows with known histories of large litters or neonatal losses) optimizes the benefit from available staffing.
Summary
The golden hour is the highest-leverage management window in the commercial pig production cycle — the period during which the gap between born-alive and weaned-alive is most directly and most consequentially influenced by the attentiveness, preparation, and technique of the person present in the farrowing house.
Each of the five interventions in this guide — airway clearance and respiratory stimulation, drying and thermal management, navel care, colostrum access assurance, and the 8-hour assessment that confirms successful transition — addresses a specific, documented cause of first-hour and first-day piglet mortality, with specific techniques that can be learned, practiced, and executed consistently by trained stockpeople.
The resource requirement is not equipment or medication — the most important interventions in the golden hour (vigorous drying, respiratory stimulation, placement at the heat source, assisted nursing) require nothing more than a clean cloth, a warm heat source that was verified functional before farrowing, and a person who knows what to do with each piglet in the first minutes of its life.
The colostrum reserve provides the safety net for the cases where the ideal is not achievable — where a sow’s production fails, where a litter is too large for fully unassisted nursing, where a piglet is too weak to nurse independently without a bridging colostrum dose that allows it to build the strength for subsequent independent nursing.
Born alive is where genetics and reproductive management deliver the piglet. The golden hour is where stockmanship keeps it.