An egg drop is a production event with a root cause. It does not occur spontaneously. When laying rate falls 10% or more below the expected trajectory, or when a flock that was performing correctly suddenly declines, something has changed in one of four domains: disease, environment, management, or nutrition.
Veterinarians and farm managers often investigate disease first. It is the most visible and the most alarming category. But nutritional egg drops caused by a deficiency in energy, a limiting amino acid, a missing mineral, or a compromised vitamin are more common than disease-driven drops in well-vaccinated flocks, produce losses that persist for weeks after the deficiency is corrected, and are frequently misdiagnosed because the nutritional gap is not visible at necropsy and does not show up in disease screening.
The diagnostic sequence matters. Treating a nutritional egg drop with antibiotics does not restore production. Reformulating a ration that is not the problem delays finding the disease that is. The investigation that reaches the right answer fastest is the one that uses the clinical picture — the pattern of signs accompanying the production drop to narrow the candidate causes before running laboratory tests or changing the ration.
This article builds that diagnostic framework: the nutritional deficiencies that cause egg drops in commercial layer flocks, the clinical signs that distinguish them, and the corrective protocols that restore production.
What a Nutritional Egg Drop Looks Like
Before diagnosing which nutrient is deficient, confirm that the egg drop is nutritional in origin rather than infectious or environmental. This distinction is made by pattern recognition, not laboratory testing — though laboratory testing may be needed to confirm.
Signs That Point Toward Nutritional Origin
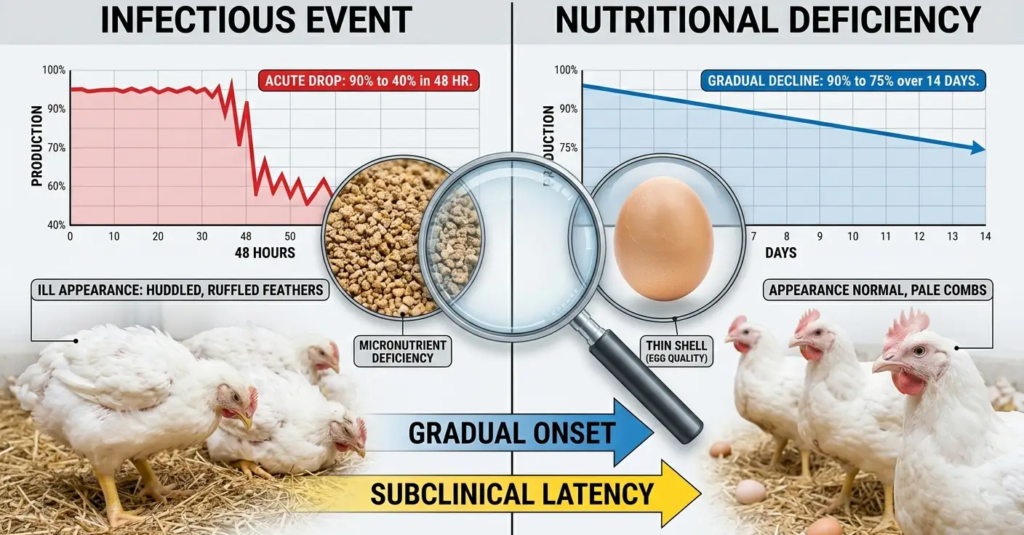
Gradual onset. Nutritional deficiencies do not produce overnight production crashes. They accumulate over days to weeks as the bird’s nutrient reserves are depleted. A flock that declines from 88% to 76% laying rate over 10–14 days is more likely to have a nutritional cause than one that drops from 88% to 55% in 48 hours.
No significant mortality elevation. Nutritional deficiencies rarely cause acute mortality. If the laying rate is dropping but mortality remains below 0.05% per day, infectious disease as the sole cause is less likely (though not excluded subclinical disease can simultaneously suppress production without causing visible mortality.
Abnormal egg quality changes alongside the rate. Nutritional egg drops frequently present with simultaneous changes in egg quality, such as smaller eggs, thinner shells, reduced albumen height, pale yolks, in addition to reduced laying rate. An egg drop with perfectly maintained egg quality suggests a non-nutritional cause, such as lighting disruption or a disease that affects ovulation without affecting the oviduct.
Feed intake deviation. A ration deficiency that is forcing birds to compensate shows up in feed intake data. Energy-deficient birds may increase intake (if the ration ME is too low and birds attempt to eat more volume). Protein-deficient or amino acid-limited birds may show no intake change despite reduced production. Any unexplained deviation from the breed-standard daily feed intake per bird is a nutritional investigation trigger.
No concurrent respiratory, neurological, or enteric clinical signs. Infectious causes of egg drops — Newcastle disease, Infectious Bronchitis, Egg Drop Syndrome 76 virus, Mycoplasma gallisepticum — almost always produce additional clinical signs: respiratory distress, enteric changes, facial swelling, behavioral abnormalities. A flock dropping eggs with no accompanying clinical signs is a nutritional or management investigation, not a disease investigation.
When to Rule Out Infectious Causes First
If the egg drop is accompanied by any of the following, rule out infectious causes before investigating nutrition:
- Mortality above 0.1% per day
- Respiratory distress, tracheal rales, nasal discharge
- Facial or sinus swelling
- Sudden drop exceeding 15% in 72 hours
- Watery or green diarrhea across more than 10% of the flock
- Shell-less or rough-shelled eggs appearing suddenly in a previously well-shelled flock
Once infectious causes are excluded by clinical assessment and, where necessary, serology or PCR, the nutritional investigation can proceed systematically.
Deficiency 1: Energy (Metabolizable Energy)
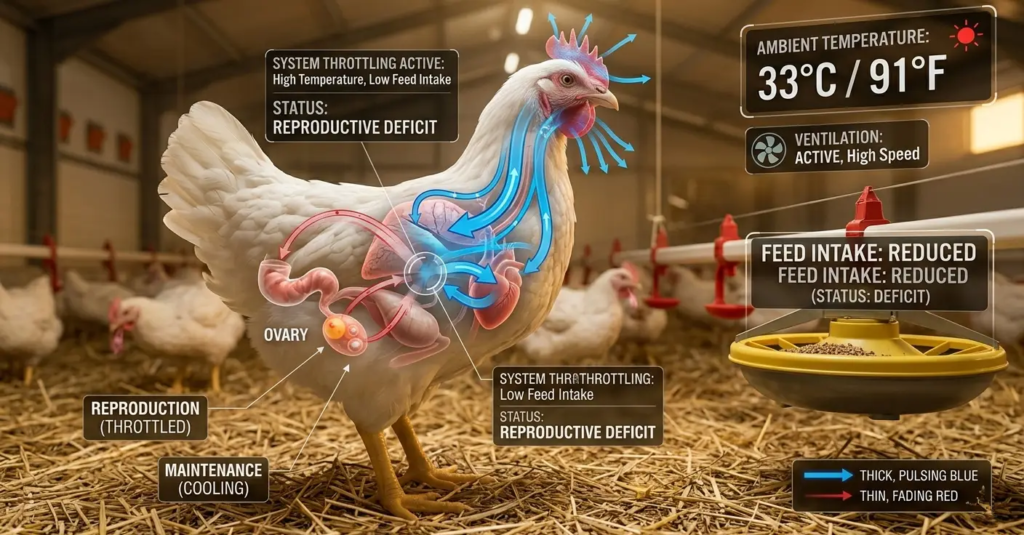
Energy is the master limiting nutrient. When a layer hen’s daily metabolizable energy intake falls below her requirement, she does not simply produce fewer eggs — she redirects energy from reproductive function toward maintenance and thermoregulation, suppressing GnRH secretion and reducing ovulation frequency.
How It Happens
Energy deficiency in layer rations in West and Central Africa almost always results from one of four causes:
Reduced ration ME below design: Local maize ME values vary significantly with variety, storage conditions, and moisture content. Maize with 14% moisture has an ME approximately 5–7% lower than dry maize at the same inclusion rate. Fat or oil supplementation omitted to reduce ration cost reduces ME below the design value. Mycotoxin contamination — aflatoxin, fumonisin, and deoxynivalenol are prevalent in stored maize in the humid tropics — reduces ME bioavailability by damaging intestinal villi and reducing nutrient absorption efficiency.
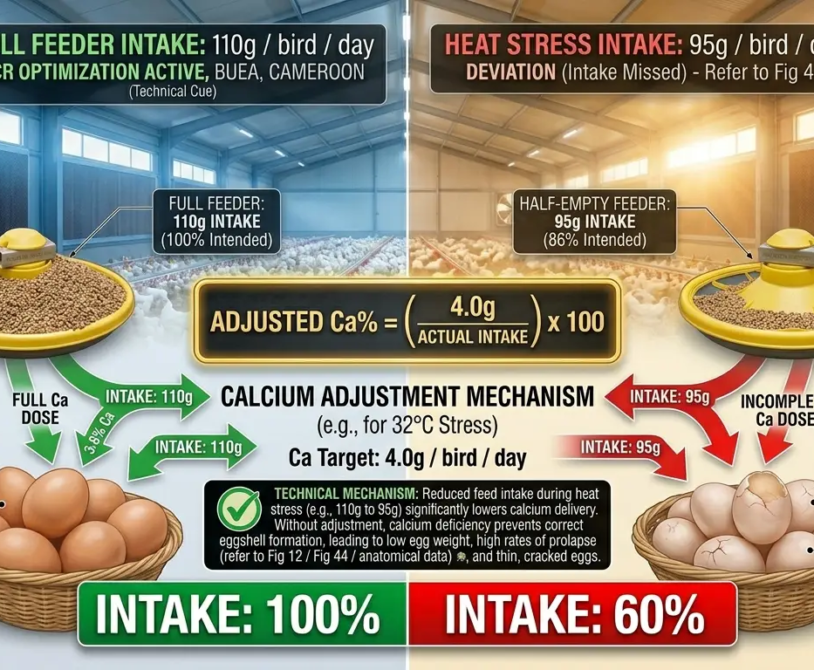
Heat stress reduces voluntary feed intake: At ambient temperatures above 28°C, laying hens reduce feed intake by 1.5% per degree Celsius above the thermoneutral zone. A flock eating 100g instead of 115g per day at 33°C ambient temperature is consuming 13% less ME daily than the ration formulation assumes. If the ration ME percentage is not adjusted upward to compensate, the hen falls below her energy requirement, and production declines.
Increased energy expenditure for thermoregulation: At high ambient temperatures, hens simultaneously reduce intake and increase their energy expenditure for evaporative cooling through panting. The energy deficit is compounded: less coming in, more going out.
The Clinical Picture of Energy Deficiency
- Gradual decline in laying rate over 7–14 days
- Body weight below the breed standard — birds in a losing condition
- Reduced fat cover over the keel bone on palpation
- Feed intake is either unchanged (if the issue is ME density, not volume) or elevated (if birds are eating more volume to compensate for low ME)
- Pale combs relative to the expected stage of lay — reduced blood flow from suppressed reproductive hormone activity
Corrective Protocol
- Measure actual daily feed intake: Weigh feed in and out for three consecutive days. Compare to the breed standard intake for the current age.
- Assess the ration ME: Have the ration analyzed at a laboratory for ME content if local ingredients are the suspected cause. Compare to design ME.
- Increase energy density: Add 1.5–3% fat (poultry fat, palm oil, or soybean oil) to the existing ration — do not reformulate from scratch initially. A 2% fat addition increases ME by approximately 50–70 kcal/kg, which closes most moderate energy gaps without reformulation.
- Apply the heat-adjustment formula if heat stress is present: Target calcium % = (Daily calcium requirement ÷ Actual daily feed intake) × 100. Apply the same logic to ME: Target ME % = (Daily ME requirement ÷ Actual daily intake) × 100.
- Address mycotoxins: Add a broad-spectrum mycotoxin binder (bentonite, montmorillonite clay, or HSCAS — hydrated sodium calcium aluminosilicate) at 0.5–1.0 kg per tonne of feed if mycotoxin contamination is suspected. Have a grain sample tested at a mycotoxin laboratory if the budget allows.
Recovery timeline: Energy-deficient egg drops typically recover within 10–14 days of correcting the energy supply, assuming no concurrent disease or structural oviduct damage from prolonged deficiency.
Deficiency 2: Crude Protein and Lysine
Protein is the second-limiting nutrient in layer production. Albumen — the white of the egg — is 88% water and 11% protein. Producing 65 grams of albumen per egg requires approximately 7 grams of protein to be secreted by the magnum tubular gland cells every 3 hours during egg formation.
When dietary protein or the first limiting amino acid lysine falls below the hen’s requirement, albumen synthesis is constrained before laying rate is affected. The result is smaller eggs at the same laying frequency — the hen continues to ovulate, but the eggs produced are lighter than they should be. As protein deficiency deepens, laying rate declines as the body prioritizes maintenance protein over reproductive protein secretion.
How Protein Deficiency Occurs
Crude protein below 16–17% in the ration: Maize-soybean meal rations formulated to cost often reduce soybean meal inclusion to reduce ingredient cost. If crude protein falls below 16% during peak lay, egg weight and then laying rate are sequentially affected.
Amino acid imbalance masking adequate crude protein: A ration with 17% crude protein but insufficient lysine (below 0.85% of ration) will suppress production even though protein percentage appears adequate. Crude protein analysis does not reveal amino acid balance. A ration can be protein-adequate but lysine-deficient if the protein sources are low in lysine relative to other amino acids.
Low digestibility protein sources: Feathermeal, blood meal, and some fishmeal sources have variable digestibility — the labelled crude protein content does not equal the digestible protein available to the bird. Rations based heavily on these protein sources may under-deliver digestible lysine relative to the formulation.
The Clinical Picture of Protein / Lysine Deficiency
- Egg weight is declining while laying rate remains stable or declines more slowly.
- Reduced albumen height (Haugh unit score declining) — thin, watery whites on candling or at break-out
- Birds maintain body weight (protein is being diverted from eggs to maintain lean mass)
- Feed intake often unchanged or slightly elevated
- No change in shell quality (calcium metabolism is independent of protein)
Corrective Protocol
- Calculate lysine intake per bird per day: Daily feed intake × ration lysine % ÷ 100. Compared to the breed standard requirement: typically 900–1,000 mg lysine per bird per day at peak lay.
- Add synthetic L-lysine HCl: L-lysine is available as a feed additive at 78–80% lysine content. Increasing the ratio of lysine by 0.10 percentage points requires approximately 1.3 kg of L-lysine HCl per tonne of feed. This is cheaper per unit of lysine than increasing soybean meal inclusion.
- Verify methionine + cystine simultaneously: Methionine is the first limiting amino acid in many maize-soybean meal rations. Target: 0.72–0.78% methionine + cystine in the ration. Add DL-methionine if below the target.
- Review protein source digestibility: If feathermeal or variable-quality fishmeal is a major protein source, replace part of the inclusion with higher-digestibility soybean meal or full-fat soya.
Recovery timeline: Egg weight response to corrected lysine and methionine is typically visible within 7–10 days. Laying rate response, if affected, takes 14–21 days.
Deficiency 3: Calcium
Calcium deficiency produces the most visible and most rapidly developing nutritional egg drop of any nutrient. Because 2.0–2.2 grams of calcium are required for every eggshell and the hen’s blood calcium pool is exhausted in hours, calcium supply failure translates immediately into shell quality failure — and then into laying rate decline as the oviduct holds eggs that cannot be calcified.
Three Scenarios of Calcium-Driven Egg Drops
Scenario A — Absolute calcium deficiency: The ration contains insufficient calcium, below 3.5% in the laying ration. Results: thin shells, soft shells, shell-less eggs appearing across the flock simultaneously. Mortality from calcium tetany may appear in severe cases. This is the easiest scenario to diagnose and correct.
Scenario B — Bioavailability failure (vitamin D₃ deficiency): The ration contains adequate calcium by analysis, but the hen cannot absorb it because vitamin D₃ is insufficient. Vitamin D₃ degrades rapidly in stored feed in tropical conditions. Rations stored for 3–4 weeks in a hot, humid feed room may deliver 65–75% of their labelled vitamin D₃ content. The shell quality failure pattern is identical to absolute calcium deficiency, but adding limestone to the ration does not resolve it. Only restoring vitamin D₃ restores absorption.
Scenario C — Timing failure (particle size error): The ration contains adequate total calcium with adequate vitamin D₃, but all calcium is supplied as fine limestone that dissolves within 2–3 hours of ingestion. During the 8-hour dark period when the shell gland is most active, the hen has no slow-release calcium source. Medullary bone is rapidly depleted. Shell quality declines progressively through the cycle — not suddenly. Thin shells in late lay that are attributed to “old hen problems” are frequently this scenario.
The Clinical Picture of Calcium Deficiency
- Thin-shelled, soft-shelled, or shell-less eggs — the proportion tracking the severity and duration of the deficiency
- Increased cracked egg rate at collection
- In severe deficiency: osteoporosis signs (reluctance to stand, fragile long bones on palpation), cage layer fatigue syndrome
- Flock-wide — not patchy (distinguishing it from individual bird reproductive problems)
- Laying rate declines following shell quality decline by 5–10 days, as oviduct retention of unshelled eggs interrupts the ovulatory cycle
Corrective Protocol
For Scenario A (absolute deficiency):
- Increase the ratio of calcium to 3.8–4.0% immediately
- Offer free-choice coarse limestone or oystershell in a supplemental feeder alongside the ration for 10–14 days — hens with calcium debt will self-select additional calcium above ration levels
- Verify feed is being consumed at the expected rate — a simultaneous feed intake problem compounds the calcium delivery failure
For Scenario B (vitamin D₃ deficiency):
- Replace the current feed batch with freshly milled feed — if storage duration is suspected, this resolves the degradation issue
- Add liquid vitamin D₃ to drinking water at 2,000–3,000 IU per liter for 5–7 days as an emergency measure while the new batch is being milled
- Increase vitamin D₃ in the ration formulation by 15–20% above standard as a safety margin for tropical storage conditions going forward
For Scenario C (particle size failure):
- Add coarse limestone (particle size 2–4 mm) at 50% of the total limestone inclusion immediately
- If oystershell is available, offer free-choice oystershell in a separate supplemental hopper — hens will select it in proportion to their calcium debt.
- Going forward, formulate all laying rations with a 50:50 fine/coarse limestone blend as standard.
Recovery timeline: Shell quality response begins within 48–72 hours of correcting the primary deficiency. Full recovery to pre-deficiency shell breaking strength typically takes 10–14 days.
Deficiency 4: Phosphorus
Phosphorus deficiency is underdiagnosed in layer nutrition because its primary effect — reduced bone mineralization — is invisible in production data until the deficiency has been present long enough to produce secondary consequences. When egg drops are associated with phosphorus deficiency, the mechanism is indirect: demineralized bones break more easily at depopulation, reduced bone strength impairs mobility and feed access, and in severe cases, the skeletal damage reduces the bird’s ability to stand at feeders and drinkers.
The Primary Pattern
- Laying rate decline is gradual and associated with signs of skeletal weakness.
- Birds are reluctant to stand or show leg weakness disproportionate to their age.
- Increased fragility of long bones — femur and tibia fractures on handling
- Poor response to calcium supplementation (because bone matrix requires both calcium and phosphorus for remineralization)
- Often appears after a prolonged period of phytase supplementation, where phosphorus was reduced below the minimum requirements without adequate monitoring
Corrective Protocol
- Increase available phosphorus to 0.38–0.40% of the ration
- Verify phytase dosage and that phosphorus reduction in the ration was not excessive — phytase at 500 FTU/kg releases approximately 0.10–0.12% available phosphorus from phytate, meaning the matrix phosphorus in the ration should not be reduced below 0.28–0.30%
- Do not reduce calcium while increasing phosphorus — the Ca:P ratio must remain in the 9–11:1 range
- Bone remineralization in a depleted flock takes 3–6 weeks — this is the slowest recovery timeline of any nutritional egg drop
Deficiency 5: Sodium and Electrolyte Balance
Sodium deficiency is a distinctive cause of egg drop that is particularly relevant in heat-stress conditions, because heat-stressed birds panting continuously lose sodium bicarbonate through the respiratory tract, creating an alkalotic state that suppresses the carbonic anhydrase activity needed for shell calcification.
How Sodium Deficiency Causes Egg Drop
The mechanism is twofold:
- Low blood sodium suppresses feed intake (hyponatremia reduces appetite directly)
- Respiratory alkalosis from heat-stress panting reduces blood CO₂ and bicarbonate, which reduces the carbonate substrate available for eggshell calcium carbonate deposition.
The result: simultaneously reduced feed intake, reduced laying rate, and thin shells — a combination that looks like an energy-calcium combination deficiency and is often treated as such without improvement.
Clinical Picture Specific to Sodium-Related Egg Drop
- Onset is closely associated with the onset of hot season or heatwave events.
- Reduced feed intake was more pronounced than expected from temperature alone.
- Shell quality decline disproportionate to calcium supply (calcium is adequate, but carbonate substrate is not)
- Water intake elevated — hens are drinking more but laying less
- Recovery when ambient temperature drops — a heat-stress association is the strongest diagnostic clue
Corrective Protocol
- Verify dietary sodium: target 0.16–0.18% sodium in the ration. Many rations are formulated to reduce salt inclusion below this level.
- Add sodium bicarbonate (baking soda) to drinking water at 0.3–0.5 g/liter during heat stress periods — this directly addresses the respiratory alkalosis and restores blood bicarbonate.
- Add potassium chloride to the ration at 0.15–0.20% during heat stress periods to support electrolyte balance (dietary electrolyte balance target: 200–250 mEq/kg)
- Feed during the coolest parts of the day (before 08:00 and after 16:00) to maximize voluntary feed intake.
Recovery timeline: 7–14 days once electrolyte balance and temperature are managed.
Deficiency 6: Key Vitamins — A, D₃, and E
Vitamin A
Vitamin A (retinol) maintains the integrity of epithelial tissues — including the mucosal lining of the oviduct. Vitamin A deficiency causes keratinization (hardening and abnormal cornification) of the oviduct mucosa, which interferes with egg formation at multiple stages: reduced magnum secretion of albumen, abnormal shell membrane formation, and reduced shell quality.
Clinical signs: Pale, dry oviduct mucosa at necropsy; increased proportion of eggs with rough or corrugated shells; reduced Haugh unit scores; increased incidence of blood spots in the albumen.
Target: 10,000–12,000 IU/kg vitamin A in the layer ration. Vitamin A degrades rapidly in the presence of rancid fat and in stored feed — use stabilized beadlet forms rather than oil-based vitamin A when feed will be stored more than 2 weeks.
Correction: Increase vitamin A supplementation. Short-term water-soluble vitamin A supplementation at 5,000 IU per liter of drinking water for 5–7 days accelerates tissue recovery.
Vitamin D₃
Covered under the calcium section above. The key corrective point bears repeating: shell quality failure that does not respond to calcium supplementation within 72 hours is a vitamin D₃ problem until proven otherwise.
Vitamin E and Selenium
Vitamin E (tocopherol) and selenium function together as the primary antioxidant defense system in the reproductive tract. Deficiency of either causes oxidative stress in the granulosa cells surrounding the developing follicle, reducing estrogen production and disrupting the pre-ovulatory LH surge.
Clinical signs: Reduced laying rate without clear egg quality changes; increased early embryonic death in fertile eggs (relevant for breeders); increased proportion of blood-streaked yolks; in severe deficiency, exudative diathesis (fluid accumulation under the skin) visible at necropsy.
Target: Vitamin E at 20–30 IU/kg and selenium at 0.3–0.5 mg/kg (use organic selenium — selenomethionine — for superior bioavailability vs. sodium selenite).
Correction: Vitamin E and selenium supplementation through the ration or water. Note that high dissolved iron in drinking water acts as a pro-oxidant that degrades vitamin E in the gut, regardless of dietary supplementation — address water iron alongside vitamin E correction if iron exceeds 0.3 mg/L.
The Nutritional Egg Drop Investigation: A Systematic Checklist
When an egg drop of nutritional origin is suspected, work through this checklist before changing any ration component. Changing multiple ratio variables simultaneously makes it impossible to identify which correction produced the recovery.
Step 1 — Confirm the drop is real: Verify egg count data is accurate. Count errors, feeder malfunctions, collection timing changes, and floor egg accumulation can produce apparent production drops that are recording artifacts. Verify three consecutive days before treating as a production event.
Step 2 — Measure feed intake: Three days of weighed feed in vs. feed remaining. Compare to the breed standard for the current age and ambient temperature.
Step 3 — Measure water intake: One day of measured water delivered vs. remaining. Target: 180–220 mL per bird per day at temperatures below 25°C, rising to 300+ mL above 30°C. Water intake below target triggers a water quality and drinker access investigation before a nutritional investigation.
Step 4 — Document the clinical picture: Shell quality changes? Egg size changes? Albumen quality changes? Yolk color? Mortality rate? Respiratory signs? Behavioral signs? Map the clinical picture against the deficiency profiles in this article.
Step 5 — Review feed batch history: When was the current feed batch milled? Has the ration formulation changed recently? Has the ingredient source changed (different maize supplier, different soybean meal origin)? Has the feed been stored in conditions that could accelerate vitamin degradation?
Step 6 — Identify the single most likely deficiency: Based on the clinical picture and feed batch history, identify the primary suspect nutrient. Correct that one variable first.
Step 7 — Measure the response: Give the correction 7–14 days before reassessing. If production recovers, the deficiency is confirmed. If production does not recover, add the next most likely deficiency to the investigation.
Step 8 — Submit feed to laboratory analysis if the cause remains unclear: Minimum panel: crude protein, ME (calculated or proximate analysis), calcium, available phosphorus, sodium. Add vitamin D₃ and mycotoxin screening if results are inconclusive.
Recovery Timelines: What to Expect and When to Escalate
| Deficiency | Expected Recovery Onset | Full Production Recovery | Escalation Trigger |
|---|---|---|---|
| Energy | 7–10 days | 14–21 days | No response after 14 days |
| Lysine / Protein | 7–14 days (egg weight); 14–21 days (laying rate) | 21–28 days | No egg weight response after 14 days |
| Calcium (absolute) | 48–72 hours (shell); 10–14 days (laying rate) | 14–21 days | No shell improvement after 5 days |
| Vitamin D₃ | 5–7 days | 14–21 days | Leg weakness has not improving after 3 weeks |
| Phosphorus | 3–4 weeks (bone) | 6–8 weeks | Leg weakness has not improved after 3 weeks |
| Sodium / Electrolytes | 7–10 days | 14 days | No response if heat stress continues unmanaged |
| Vitamin A | 10–14 days | 21–28 days | Shell texture abnormalities persisting after 14 days |
| Vitamin E / Selenium | 14–21 days | 28 days | No laying rate response after 21 days |
If a flock does not respond to a correctly identified and correctly corrected nutritional deficiency within the expected recovery window, two possibilities exist: the deficiency identification was incorrect, or there is a concurrent cause (infectious disease, structural oviduct damage from prolonged deficiency, or a toxin load) preventing recovery. Submit samples for laboratory investigation if any correction is not producing the expected response within its recovery window.
Summary
Nutritional egg drops are diagnosable by clinical pattern, correctable with targeted interventions, and recoverable within defined timelines — if the investigation follows a systematic sequence rather than defaulting to antibiotic treatment or ration-wide reformulation.
The clinical picture — the specific combination of shell quality changes, egg size changes, laying rate trajectory, feed and water intake deviations, and absence or presence of concurrent clinical signs — is the diagnostic instrument. It is more useful, faster, and cheaper than laboratory analysis as the first step. Laboratory analysis confirms the diagnosis. Clinical pattern recognition identifies it.
An egg drop is not an emergency in itself. It is a signal. Read the signal correctly, trace it to the right nutrient, correct that nutrient specifically, and measure the response. In the vast majority of cases, the flock recovers within three to four weeks.
The farms where egg drops become production crises are the farms where the signal was treated with the wrong response — and the right response was found only after the wrong ones failed.